
Background
The Alex Community Health Centre (CHC) in Calgary, Canada serves a diverse array of community members vulnerable to poor health outcomes. Social innovation in this setting helps the community solve their own complex problems, but in doing so also offers an empowering moment where they can experience the dignity of their own power and resilience. This is predicated on the concept of agency, of having control of one’s life, being an important determinant of health.1,2
The Alex CHC has been an innovative organization from its early days. Established in 1973, in a small basement in a low-income neighborhood, it has grown into a wrap-around complement of services that solve both health and social challenges. In addition to a team of physicians at youth, family, and senior clinics, there are social workers, case managers, nurse practitioners, and housing specialists. Beyond the medical centers, there is a Community Food Centre that focuses not only on healthy eating but also relationships and social justice. There are three housing first programs within the organization that are helping those who are homeless at the intersection of mental health diagnoses. Patients often suffer from multiple chronic diseases in the context of social isolation. Many have experienced addictions, housing and food insecurity, and have a history of adverse childhood events.
The field of social innovation had not been explored through any local CHC, and the intention was to conduct a pilot (prototype) to learn how it might benefit the community. The facilitator (author), space, and materials were provided by The Alex CHC. Further funding is outlined below.
Methods
The Solutions Studio (Studio) was launched in October 2017 with an initial focus on mobility, as this is known to be an area where agency can prove beneficial from a public health perspective.5 Community members who had challenges in this realm, using a walker or wheelchair, were invited to participate, with the intention of hosting between six to ten participants. The meeting was opened to both the Family and Seniors Clinic patients, and nine people joined in the first session.
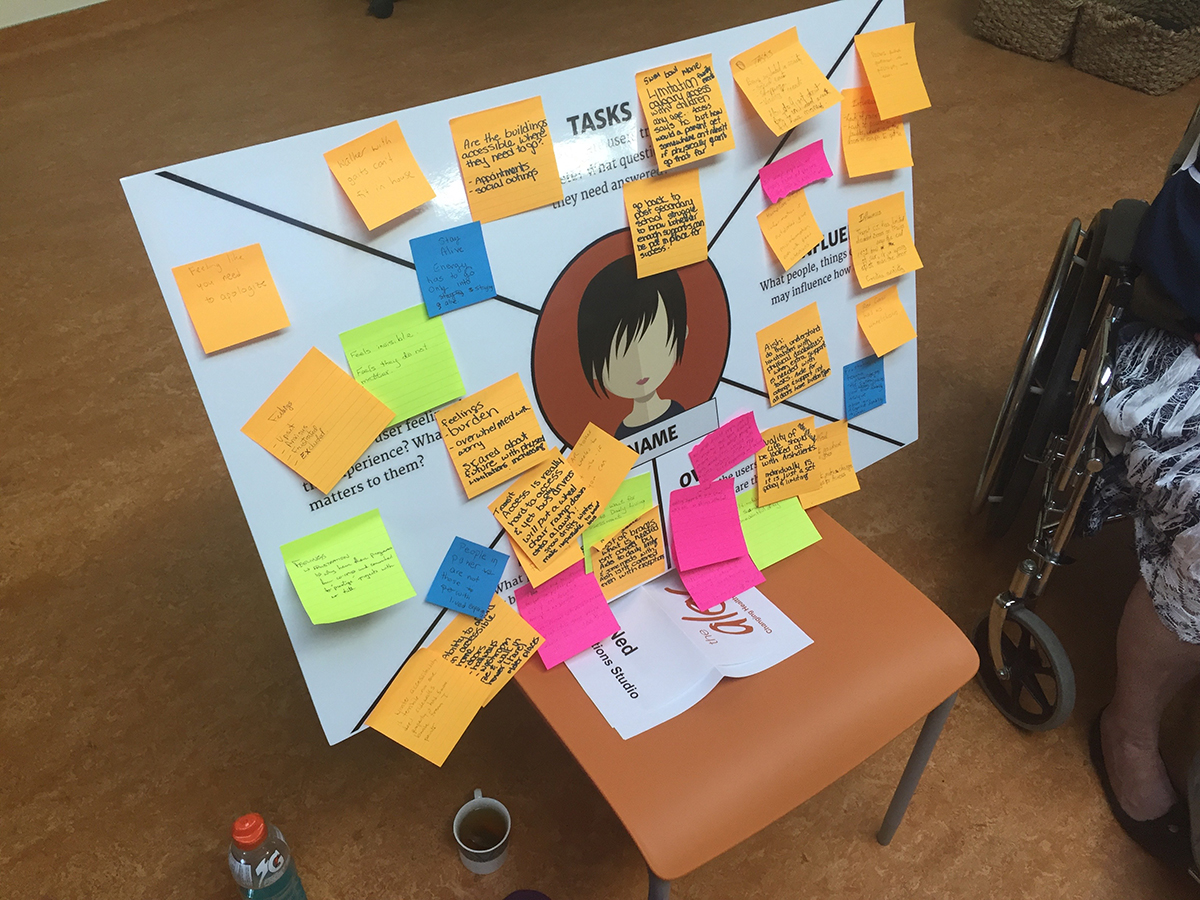
Participants were taken through a three-step process, an abbreviated version of traditional social innovation labs.3 In the first step, they used an Empathy Map to establish the lived experience of a hypothetical person who was dealing with mobility issues (see image 1). They discussed feelings, goals, pain points, tasks, and influences of this imaginary person. This step took the pressure off each participant to appear vulnerable about their own story. In this way, they approached the rest of the session from the point of view of an invented scenario that was collectively created. The Solutions Studio Mobility Group described a person who faced many systemic challenges throughout their day, including multiple barriers to adapting to the environment where they live and carry out the activities of daily living, who often was left feeling hopeless and frustrated as a result of their need. The group described the intersectionality of poverty and housing insecurity due to the lack of affordable, accessible options.
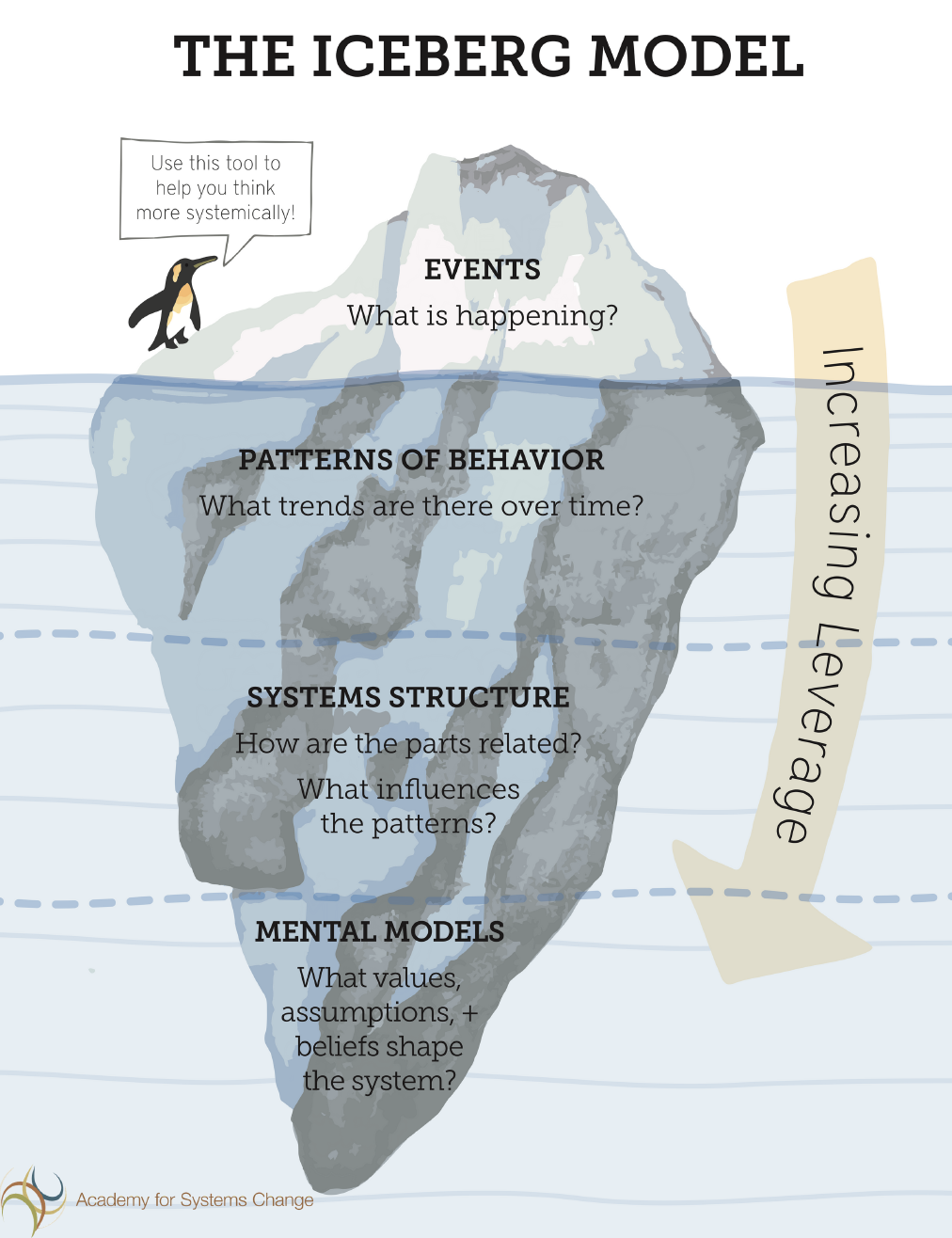
The second step in the process was the use of an Iceberg Model of systems leveraging4 (see image 2). This tool enables an emergent deepening of leverage points within systems, starting from the inciting event to the superficial trending patterns, to change within policy or structures, and what would potentially be most sustainable through mental model shifts. They spent some time discussing possible leverage points for this hypothetical person that they had manifested through the Empathy Map exercise. Using the Iceberg Model, our community members brainstormed the third step, where they each came up with solutions and then discussed them as a group. Solutions were ranked from easy to complex and from individual to system-level.
Results
The Solution Studio Mobility Group came up with a myriad of solutions that would be very difficult for those without lived experience to envision. For example, at the level of a solution that was midway between “easy to complex” and between “individual to systemic,” they decided to film and edit a video that would demonstrate to key stakeholders how difficult it is to navigate the city streets in Calgary. Especially in wintertime, inconsistent snow removal and the need for low-income patients to use public transit, can cause people to remain at home due to fear of safety. This leads to enhanced social isolation among a group who often has difficulty making it to appointments for medical or psychosocial reasons. Participants used the Iceberg Model to determine how to leverage opportunities and decided to make the video aimed towards our municipal councillors – to ask for an “accessibility audit” of the buildings and to ask for their participation in a “take a wheelchair to work for a day” event.
Other proposed solutions included calling the city’s non-emergency services line to describe the conditions of their public transit or sidewalks (simple, individual). They recommended organizing co-operative housing units where single mothers, those with various disabilities, and the elderly could cohabitate to solve each other’s problems rather than rely on strangers through paid or public caregiving (complex, systemic).
There has not yet been a formal evaluation of the process yet, as it was deemed that the existing metrics to measure self-empowerment might not be an adequate reflection of any potential benefit,6 and it has been less than a year since we began meeting. The group meets with their facilitator (the author) monthly and has been awarded a $750 CAD ActivateYYC grant through the City of Calgary’s Innovation Fund to make their video that is a work-in-progress.
The second Studio was held in February 2018 and focused on the theme of chronic pain. There were six people who attended and interestingly all participants were male. One of their requests was to form a men’s support group for this condition, as they felt that it is difficult for men (and those who identify as male) to express mental or physical pain in our society. This was done within the week and has been well-attended by both the men from the Studio and others in our community. They asked for many other medical and research interventions, around medical marijuana and more, which are underway or currently being researched for collaborative opportunities.
A third Studio is planned for the fall of 2018, with the topic of Addiction and Recovery. Afterwards, in partnership with our Community Food Centre, we intend to try larger facilitated table-groups to go through the process around Poverty Reduction.
Discussion
The Solutions Studio experiences at The Alex CHC in Canada demonstrate that through facilitation of a social innovation lab process, community members can generate inventive solutions to their complex challenges. For health care administrators or primary care providers, often these solutions would not come to mind, as we generally lack the lived experience.
Outcomes of the social innovation lab are, by definition, desired by the community being served, and thus more likely to be effective solutions to suit their needs and context. One common complaint of existing health systems is a lack of understanding of the determinants of health that influence illness experiences. Solutions Studio’s focus on the Empathy Map process allows those suffering from these conditions or circumstances with an opportunity to share their experiences thus providing additional knowledge to health care professionals and ultimately a learning opportunity for all.
Since it was a physician facilitating the Studio, any triggering events due to traumatic topics were handled clinically. The solutions that involved medical interventions could be guided through this lens. Participants were noted to express trust, given a primary care provider was listening and acknowledging their stories. However, there is also the possibility that having a physician lead the process could create friction for those who have not had good experiences within the health care system. There have been many instances of vulnerable community members being treated without respect or made to feel powerless. Thus, the facilitator made many mentions of privilege in the context of her role and their power to make change. It is hoped that once sufficient members of The Alex’s patient-base have gone through the process, confidence in the organization and greater systems might be achieved. Any forthcoming policy changes at the institutional or government level would be further proof of their collective agency.
The model works, as community members, even those who are marginalized or have low literacy, are capable of understanding this simplified process. When their proposed solutions become tangible, it provides a crucial sense of agency that is often lacking in this population. We have been informally collecting narrative experiences of the Studio members, and they have been positive. Our hope is to involve University students to generate a narrative-focused research project to learn more about how the process can be further refined and scaled. A developmental evaluation process using principles-focused evaluation may be best suited for this stage in the innovative process.7,8
Endnotes
1. Abel T and Frohlich K, “Capitals and Capabilities: Linking Structure and Agency to Reduce Inequalities” Soc Sci Med. 74,2 (2016): 236-244
2. Rutten A and Gelius P, “The Interplay of Structure and Agency in Health Promotion: integrating the concept of structural change and the policy dimension into a multi-level model and applying it to health promotion principles and practice” Soc Sci Med. 73, 7 (2011): 953-959
3. Social Innovation Lab guides available for download through http://www.sigeneration.ca/home/labs/ accessed July 26, 2018
4. Image 2 was downloaded from the Academy for Systems Change website from donellameadows.org/systems-thinking-resources/ accessed July 26, 2018
5. Blacksher E and Lovasi G, “Place-focused Physical Activity Research, Human Agency, and Social Justice in Public Health: taking agency seriously in studies of the built environment” Health Place. 18, 2 (2012): 172-179
6. Ibrahim S and Alkire S, “Agency and Empowerment: A Proposal for Internationally Comparable Indicators” Oxford Dev Stud. 35,4 (2007): 379-403.
7. Patton, Michael Quinn. Developmental Evaluation.
8. Patton, Michael Quinn. Principles-Focussed Evaluation.
Author Bio
Dr. Christine Gibson is a family physician who has a special interest in medical education and in health inequity. As part of a master’s in medical education, she created the Global Health Enhanced Skills training residency in the Department of Family Medicine at the University of Calgary. She is Executive Director and Founder of Global Familymed Foundation, a nonprofit that works with international academic partners to support the training of generalist physicians to practice where they are needed most. As a Social Innovation Wellness Specialist, she looks to create a niche of positive deviance within her work environment at The Alex Community Health Centre. Click here to view her TEDx talk from 2015 after being caught inadvertently in the earthquakes in Nepal.