
By Charles Nyasa (BSc. PT, Honors),1 Anthony Mwakikunga (PhD. Anatomy),1 and Enock Chisati (MSc. Ex Phys & Spo)2
1 Division of Anatomy, Department of Biomedical Sciences, University of Malawi College of Medicine, Blantyre Malawi
2 Department of Physiotherapy, University of Malawi College of Medicine, Blantyre, Malawi
Background
Malawi, officially known as the Republic of Malawi, is a small country located in the south-eastern part of Africa. It is bordered by Mozambique on the west and southwest, by Tanzania on the north and northeast, and by Zambia on the west and northwest. (United Nations 2017) Covering 118 484 sq.km of land and water surface area, (United Nations 2017; MoH 2017) the country boasts a rich cultural heritage, fertile soils that favor agriculture (the major driver of the country’s economy), beautiful landscapes (such as Mulanje Mountain and Lake Malawi, the third largest of the East African Rift Valley) and abundant flora and fauna (Figure 1). Malawians are characteristically warm, friendly, and peace-loving, and unmistakably, the country is branded the warm heart of Africa.
Three major regions, the northern, the central, and the southern, demarcate the country. These regions are administratively further demarcated into 28 districts; six in the northern region, nine in the central region, and 13 in the southern region (Figure 1). (NSO 2018; MoH 2017) According to the National Statistics Office (NSO), Malawi now has a population of about 17.5 million, reflecting a 35 percent increase since 2008. (NSO 2018, 2008) 49 percent of total population is comprised of females, and the southern is the most populous region holding about 44 percent of the people, followed by the central region (43 percent), and the annorthern region (13 percent). About five percent of people in Malawi are more th 60 years old, also reflecting an absolute rise since 2008. (NSO 2018)
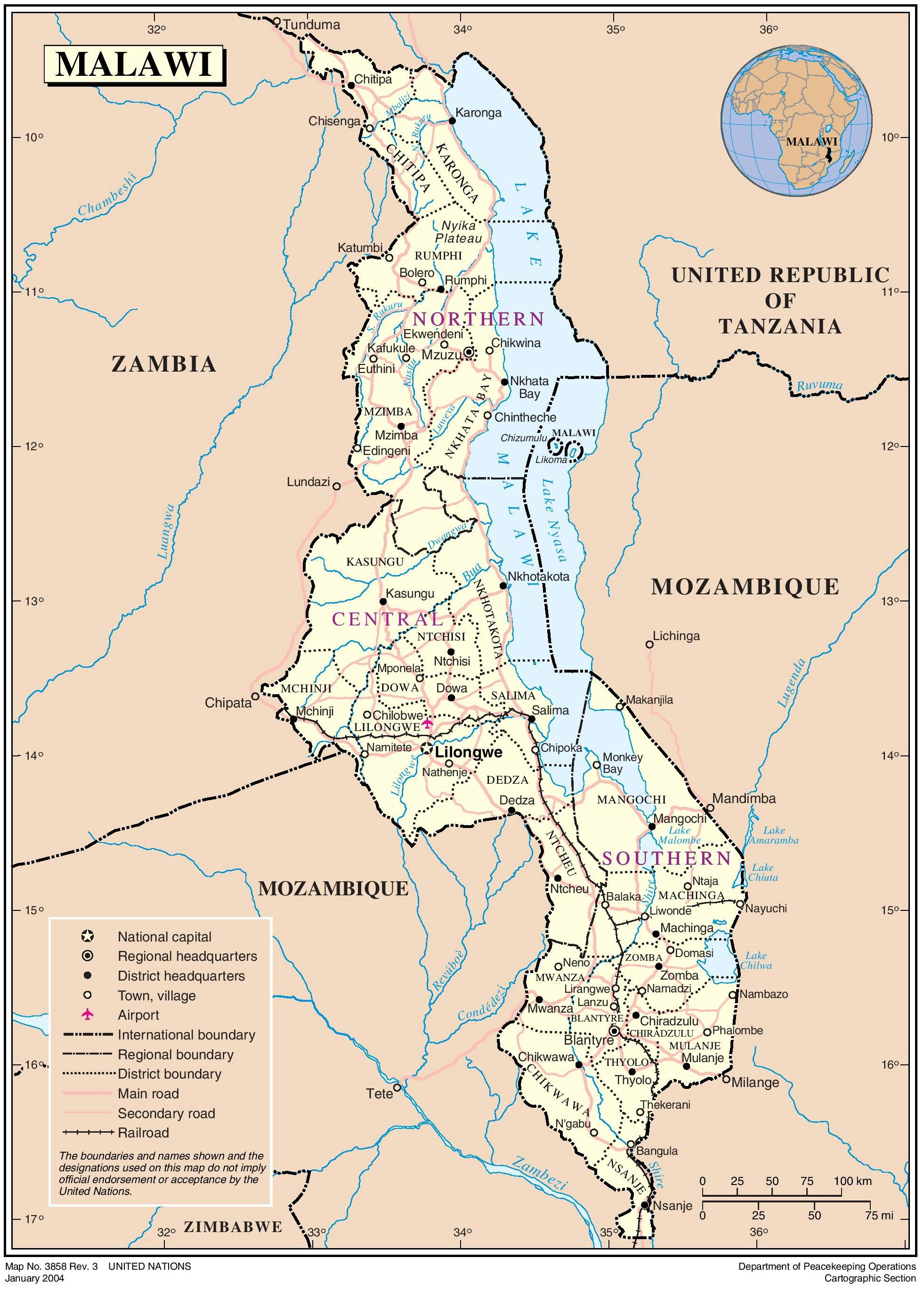
Figure 1: Maps showing the location of Malawi in Africa, as well as regions (northern, central and southern) and districts of Malawi. Source: www.mw.one.un.org
The population of Malawi is predominantly rural based and youthful. More than 84 percent of the population live in rural areas and 51 percent of the people are below the age of 18. Life expectancy is estimated at 58.4 for both sexes in 2017. (MoH 2017) Further, about 91 percent of elderly people live in the rural communities. (NSO 2018) In an economic sense, the significant proportion of the youth is seen as a precious resource which if properly cultivated may help accelerate and sustain the country’s economic and political development. (United Nations 2017) From another angle, the rising number of older people in Malawi, though often perceived as a disadvantage, also carries with it, ingredients for potential realization of overall development goals.
Being a low-income and predominantly agriculture-based economy (GDP per capita estimated at US 381.40, as of 2015), (MoH 2017) life is generally hard for an average person. This is even worse among those who are unfavorably positioned in the society, either due to age, disability, or other social inequalities. Older people are usually faced with double or triple disadvantage. This is mainly because of age-associated declines in functional ability which hinder potential to maintain gainful employment as well as the higher likelihood of disability and reduced levels of community participation as people age. (WHO 2015) These in turn place a huge burden on the country’s economy due to over-utilization of essential social services such as health care and inability of the nation to fully realize the benefits of population ageing.
Health care Delivery in Malawi
In Malawi health care services are provided by public, private-for-profit (PFP), and private-not-for-profit (PNFP) sectors. (MoH 2017; Makwero 2018; MoH 2012) Public health care services are provided mainly through the Ministry of Health in collaboration with district, town, and city councils, Ministry of Defense, Ministry of Internal Affairs, and Public Security (police and prisons) as well as the Ministry of Natural resources, Energy and Mining. (MoH 2017) The PFP sector comprises private hospitals and community clinics, which according to Makwero, (Makwero 2018) are mostly rudimentary, and lack coordination and regulation. These aim to provide curative services and laboratory services, to a minimal level. The PNFP sector comprises mission and non-governmental health facilities the major player, providing about 29 percent of all health services in Malawi, being the Christian Association of Malawi (CHAM). (MoH 2017; Makwero 2018) Unlike PFP and PNFP services, public services are provided free of charge at the point of access. However, from time to time, government through the Ministry of Health works hand in hand with private sector facilities to deliver various components of Primary Health Care (PHC), mainly through Service Level Agreements.
All these facilities are virtually for the general population and there are no known public or private facilities specially designated for the elderly in the country, except for a few low-level community initiatives that are mainly attached to operations of select charity organizations. In addition to that, although there may be special wards and sections for children or pregnant mothers at almost all levels, there are no similarly designated sections for older people at any level and no deliberate policies are in place to promote and improve accessibility of facilities and services for this population group. This is despite well-established knowledge drawn from day-to-day clinical experiences that older people are prone to serious health, psychosocial, and cultural issues that differ significantly from other population groups thereby requiring special attention. However, Government of Malawi recognizes the influence of health status on an older person’s capacity to earn a living and participate in family and community life, and through the National Policy for Older Persons (2016), (National Policy for Older Persons 2016) commits to introduce elderly-friendly health services and lobby for inclusion of geriatric health services in existing health facilities in order to improve management of chronic diseases associated with ageing. Currently, this is still not explicitly reflected in the National Health Sector Strategic Plans II, 2017-2022 (HSSP II). (MoH 2017)
In terms of health service delivery, Malawi has a three-tier system comprising primary (community initiatives, health posts, and rural hospitals), secondary (district and CHAM hospitals) and tertiary level (central hospitals) institutions. (MoH 2012; WHO 2018) These are linked to one another through a comprehensive referral system. (Makwero 2018; MoH 2012; WHO 2018) There are four central hospitals in Malawi namely; Mzuzu Central Hospital in the Northern region, Kamuzu Central Hospital in the Central region and Zomba and Queen Elizabeth Central Hospitals in the Southern region.
Some governmental sources, however, portray Malawi’s healthcare delivery system as a four-tier channel. (MoH 2016) These publications recognize the community level of care which comprises the work of Health Surveillance Assistants (HSAs) as a stand-alone level. HSAs work to compliment health posts and rural hospitals mainly by providing promotive and preventive services through door-to-door visitations under the supervision of Senior HSAs. Although this is the case, in the HSSP II the Ministry classifies the work of HSAs as under primary level of care. (MoH 2017) Nevertheless, the incorporation of HSAs in the MoH service-delivery chain maybe a resource for streamlining healthcare access for community-dwelling order adults who are aging in place, particularly those that cannot manage to walk a distance of over eight km to access a health center. At this time, this opportunity is yet untapped.
While Malawi’s tertiary-level institutions are designed to provide advanced specialist services at regional level as well as provide referral services for district hospitals within a region, primary, and secondary level facilities are tasked to address components of the Primary Health Care as is stipulated in the Declaration of Alma Ata. (Declaration of Alma-Ata 1978; MoH 2017) However, in reality about 70 percent of all services provided by tertiary-level institutions are either primary or secondary level services. (MoH 2017) This has been argued to be in part due to lack of gate-keeping mechanisms at lower levels of care. (MoH 2017; Makwero 2018; MoH 2016)
In Malawi, PHC services are delivered through the Essential Health Package. (Declaration of Alma-Ata 1978) Instituted in 2004 as a modification of PHC, the EHP is a prioritized but limited package of basic and cost-effective health services (delivered free-of-charge at the point of use) determined on the basis of scientific and practical experience and its ability to significantly impact the health status of the majority of Malawians. (Makaula et al. 2012) The aim of the EHP has been to address the burden of disease by delivering cost-effective interventions that target the top diseases and conditions in terms of burden of disease. (MoH 2017) As such, EHP obviously did not adequately embrace all components of PHC, neither did it include interventions for all known diseases across the lifespan.
Over the years, partly due to various limitations of existing packages, the EHP has undergone revision. The HSSP II currently brings with it a revised version of the EHP, known as the Basic Health Package (BHP). One problem with this current package however, is that during its development the concept of equity (in which case an intervention was recommended for inclusion in the package based on whether it targeted at-risk and marginalized groups) was considered with bias towards women and children under-five alone while neglecting the elderly (another at risk and marginalized population group). For instance, the list of interventions in BHP is loaded with antenatal care, modern family planning, child delivery, essential vaccines and childhood illness management components. (MoH 2017) Even all components under nutritional interventions are targeting only women and children under-five. Except for Tuberculosis, the BHP does not cover interventions for chronic diseases. Finally, although the package includes interventions for Non-Communicable Diseases (NCDs) (which are the most prevalent disease forms among older people), such interventions are merely in forms of promotive and preventive service such as basic psychological support, advice and follow-ups. (MoH 2017) It is only unfortunate that this is happening at a time when Malawi is undergoing an epidemiological transition in which the burden of NCDs is rising. Coupled with increase in life-expectancy and the seemingly-higher likelihood of multiple pathologies as people age, this means that more Malawian will get to live longer but disease-burdened. In this case, such interventions as rehabilitation and physiotherapy are currently an urgent need.
However, the government appears to have also recognized this issue. This is demonstrated in that aside the BHP, the MoH also developed a more comprehensive and somehow responsive package called the Basic Health Package Plus (BHP+) as an aspirational package intended to guide any future increase in resources towards desired interventions which are currently unaffordable. (MoH 2017) Unlike the BHP, the BHP+ includes comprehensive interventions for chronic diseases and some conditions prevalent as people age. However, this is not operational at the moment as it awaits availability of more resources.
Welfare of older people in Malawi
Older people constitute the fastest growing population segment worldwide. (Multani and Verma 2007) This is for several reasons, among them increase in life-expectancy and reduced fertility levels. (Hagen 2009) Although Malawi’s population structure is more youthful than most other countries (especially developed countries), statistical projections show that Malawi, just like other African nations, will soon follow suit. (United Nations 2017) In response to this, government has, during the past two decades, taken a number of bold steps targeted at promoting the welfare of older people in Malawi. These have included, establishment of the (then) Ministry of Disability and Elderly Affairs and the Bingu Silver-Grey Foundation during the reign of late President Bingu wa Mutharika, the signing of the Livingstone Call for Action on Social Protection in 2006, inception of the National Policy on Social Protection and subsequent roll out of pilot social cash transfer schemes among the vulnerable which to a huge part also included the elderly. (Hagen 2009; Nyondo 2014) However, as is the case with most presidential initiatives in the country, most of these projects have lost their momentum following the changes in state leadership. (Nyondo 2014) In 2016, Malawi enacted the National Policy for Older Persons in Malawi. The policy acknowledges the overall poor quality of life among older people in Malawi and makes commitment to mitigate such, particularly by strengthening social protection programmes, improving access to health care and provision of housing and shelter, among other objectives. (National Policy for Older Persons 2016)
There is evidence that most older Malawians live in poverty, have poor health and nutritional statuses, have no home or shelter and are often abused. (National Policy for Older Persons 2016; Hagen 2009) In a study on living arrangements and health at older ages in rural Malawi, Kendall et al, found low average mental health (50.9 – 55.2 out of 100) and physical health (47.6 – 50.6 out of 100) scores among men and women aged 45 years and above. (Kendall and Anglewicz 2018) Prevalence of falls and other geriatric syndromes in Malawi was reported in a 2014 study by Allain, et al. (Allain et al. 2014) In this study, 41 percent and 25 percent of adults aged at least 60 years old had fall problems and urinary incontinence respectively. (Allain et al. 2014) Furthermore, about 66 percent of the participants reported having memory issues, reflecting a common but unrecognized problem.
At international level, literature suggests that a significant proportion of older adults in Africa face discrimination. (WHO 2015) In Malawi, this discrimination is faced at family, community as well as national levels, particularly when accessing various essential social services. Older Malawians are often thought of as dependents and economically challenged hence not contributing much to the economy of the country. These persistently-stubborn stereotypic perceptions are further fueled by ageist terms that have for long flooded demographic literature. For example, terms such as age-dependency ratio, defined as the ratio of older dependents to the working age population, assume that everyone between the age of 15 and 65 works while everyone above 64 is dependent and exclusively relies on the productivity of younger generations. (WHO 2015) In turn, health practitioners working in low-resource settings have often appealed to these ageist stereotypes and prioritize younger people at the expense of older ones. This is most likely to be observed in settings where the rarest forms of medical care such as dental care, surgery and physiotherapy are meant to be accessed. Further, the general design vis-à-vis poor accessibility of health care facilities, non-existence of long-term care facilities, lack of designated geriatric sections in public hospitals, (Twea 2016) and delays in implementation of elderly social protection programs, (Nyondo 2014) all point to the same issue. What these reflect is that when formulating polices and allocating budgets, ageing-related matters compete with issues related to other population groups (such as youths, women of child-bearing age, children, and athletes) and often end up being marginalized. (Kazeze 2008)
Recently, The World Health Organization (WHO) has demonstrated the many flaws that are associated with measures such as age-dependency ratio as well as their discordance with proposed SDG agendas and has condemned its use to the strongest terms. (WHO 2015) Based on its recommendations, policy makers are encouraged to look at population ageing as an investment having both costs and contributions. People of Malawi should look at ageing as a two-way inter-dependence between the young and the old. Government on the other hand, should focus on putting in place mechanisms to that facilitate cultivation of older people’s potential for overall economic development. Now, it is realized that investing in older people’s health and long-term care has the potential of improving functional ability and therefore capacity to keep a job, increases agricultural productivity, puts less pressure on a nation’s health system, and lessens the burden of caregivers allowing them to do other economically-productive things. (WHO 2015)
Experiences at Kalibu Elderly Clinic
To the best of the authors’ knowledge, Malawi has only two dedicated elderly care facilities; Newlands home for the elderly and Kalibu elderly clinic both of which are located in Blantyre District. Unlike Newlands home which is a paying facility designed to accommodate white people only, Kalibu elderly care facility provides free-at-point-of-use health care services to all Malawians aged above 59 years. (Kalibu Ministries 2016) Located in the rural outskirts of Blantyre District, the clinic was established in 2014 by the order of Kalibu ministries to augment government’s efforts in promoting healthcare access among the elderly. (Twea 2016) As of 2014, the clinic was providing care to more than 800 older persons from within Blantyre District, as well as other surrounding districts including Nsanje, Balaka, Neno, Mwanza and Zomba (Figure 1). (Kalibu Ministries 2016) Currently, numbers are reported to have increased to over 2000 (Kalibu Elderly Clinic records). Being a facility established to serve the population of typical community-dwelling older Malawians, the authors are of the view that experiences at Kalibu Elderly Clinic can give a clear picture of the health characteristics of older people in Malawi.
Operation-wise, Kalibu Elderly Clinic is an Out-Patient Department (OPD) facility and comprises medical section, nursing section, dental unit, a pharmacy and a department of physiotherapy. On a daily basis, the clinic’s healthcare team assists clients who come to the clinic during morning hours. In the afternoon, the team embarks on an outreach program to follow up on clients who, for various reasons ranging from frailty to disability, may not be able to visit the clinic. This helps widen the clinic’s care circumference and ensures older people maximal benefit from the facility.
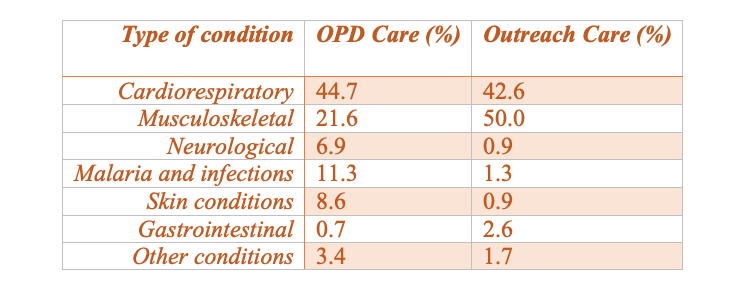
Based on records, cardiorespiratory and musculoskeletal conditions as well as infections constitute the major presenting complaints among clients who report for OPD and outreach care at the clinic. (Table 1) The higher prevalence of musculoskeletal conditions observed (21 percent of OPD cases and 50 percent of outreach cases relates well to findings of a Blantyre-Malawi study, in which falls were one of the major geriatric giants reported in more than 41 percent of instances. (Allain et al. 2014) It is suggested that mobility problems due to musculoskeletal defects such as muscle weakness, poor balance, and foot problems are a risk factor for falls among the elderly. (Multani and Verma 2007; National Center for Injury Prevention and Control 2008)
Table 1: Summary of types of medical conditions among OPD and Outreach care clients at Kalibu Elderly Clinic. Source: Kalibu Elderly Clinic records.
At times, patients are referred from the facility to surrounding health centres (such as Lilangwe Health Centre) and hospitals (particularly, Queen Elizabeth Central Hospital) for continued care. (Twea 2016)
Social contributions and needs of older people
In the past, particularly in Africa and Asian countries, older people used to depend on the economic and social support of their prime-aged children and the community. (Hagen 2009; Kazeze 2008) This traditional welfare system was housed the extended family network where family members were looking for each other and provided food, shelter, and protection for those members who were unable to provide for themselves. (Hagen 2009) For instance, prime-aged adults took care of their parents and children. In turn, grandparents and old people had the knowledge, wisdom, and skills to pass on to younger generations. This was the case in Malawi. (Kazeze 2008) In those times, older people had control over a family and their contributions to society were easily discernible. In the recent years though, due to labor migration, demographic changes, and westernization, the extended family network has been seen to weaken. (Hagen 2009; Kazeze 2008) The changes in family ties and the difficult economic situations have made it hard for children to look after their ageing parents, a thing which has made their very existence a liability.
Several studies have revealed multiple ways through which older people contribute to socio-economic development at family, community, national as well as international levels. (WHO 2015; Kazeze 2008; Hagen 2009) In developed countries, older people contribute to economic development through increased consumption and taxation, participate actively in formal workforce, and are key sources of cash flow within families where income and assets are usually transferred from older family members to younger ones. (WHO 2015) For instance, in United States, people older than 55 control more than 70 percent of all disposable income. Furthermore, it is estimated that those older than 55 will be responsible for two-thirds of all increased consumption between 2015 and 2030 in France. (WHO 2015)
In African countries, on the other hand, older people are seen to contribute to national development through increased agricultural production, active participation in both formal and informal workforce, and raising of children whose parents may have migrated to search for jobs or may have died, in most cases as a result of the HIV and AIDS pandemic. (WHO 2015; Hagen 2009) For instance, the average age of farmers in Kenya is 60 years, (Aboderin and Beard 2015) and the case might be similar for most other agriculture-dependent economies such as Malawi. From a global development point of view, the beneficial aspects of aging can be seen as potential hook-points for progression towards achievement of Sustainable Development Goals and therefore need to be cultivated by every nation.
In Malawi, issues of older people are addressed by the Ministry of Gender, Children, Disability and Social Welfare, (formerly, Ministry of Disability and Elderly Affairs) whose inception demonstrated government’s commitment towards improving the welfare of older people in Malawi. The efforts of the ministry are further supported at community levels by a number of usually small organizations and projects which are overseen and umbrellaed by the Malawi Network for Older Person’s Organization (MANEPO). Most of the works of the ministry and its partner organizations focus on responding to social challenges facing the elderly in communities, such as introduction of cash transfer programs to minimize poverty and initiation of farm input subsidy schemes to increase food security and improve nutrition. (Kazeze 2008)
However, addressing issues of the elderly is not the same as addressing the issue of population aging. This is because ageing is not a social circumstance experienced by only a fraction of the population but a universal reality of our society. With the rise in life-expectancy, it can be supposed that everyone will get old eventually and ageing will always be there all the time. Therefore, instead of putting effort to address individual ageing-related issues as they come, focus should be put on cultivating the potential of the elderly, particularly through investments in their health and long-term care with aims to maximize older their functional ability, potential to maintain gainful employment and health-related quality of life. This would in a long run translate into increased consumption, increased agricultural productivity, enhanced capacity for knowledge transference, less burden on the country’s health system, (WHO 2015) and on overall, maximum benefit from contributions of older people in Malawi.
Way Forward
The Nation of Malawi needs to prepare for the surge in population aging that is coming. Government and policymakers need to revise and introduce policies that view the relationship between younger and older populations as a two-way interdependence having both costs as well benefits. Environments that allow older people to fully participate in family as well as community activities and contribute to social economic development of the nation need to be created. To do this, high-quality data that seek to understand the current quality of life and health characteristics of older Malawians is therefore required to adequately inform policy on a broader perspective and allow effective implementation of intervention programs on ground.
The national policy for older persons highlights absence of comprehensive information about the situation of older persons in Malawi and recognizes the same as one of the major factors that make responding to the needs of the growing population of older persons in the country difficult. (National Policy for Older Persons 2016) The same problem was identified by Allain et al. (Allain et al. 2014) As such, in its implementation strategies, Government, through the ministry responsible committed to promote development of research agendas for the elderly sector and dissemination of research findings on aging, among other actions. (National Policy for Older Persons 2016)
In response to the call, a research project on evaluation of functional capacity, physical activity levels, and health-related quality of life among community-dwelling older people in Malawi (which this piece of writing is part of) is currently underway. The authors believe that such information provides a firm step towards introduction of policies that position older Malawians more favorably in the society in as much as healthcare access, maximization of functional ability and improvement of overall quality of life are concerned. Further, it will inspire other professionals to develop interest in issues of population ageing. However, more collaborations are needed across sectors (universities, health institutions, non-governmental organizations, and the ministry) in order to improve quality of life for older persons in Malawi.
Conflict of Interest Statement
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Works Cited
Aboderin, Isabella A.G., and John R. Beard. 2015. “Older People’s Health in Sub-Saharan Africa.” The Lancet 385 (9968): e9–11. doi.org/10.1016/S0140-6736(14)61602-0.
Allain, T. J., M. Mwambelo, T. Mdolo, and P. Mfune. 2014. “Falls and Other Geriatric Syndromes in Blantyre, Malawi: A Community Survey of Older Adults.” Malawi Medical Journal 26 (4): 105–8.
Declaration of Alma-Ata. 1978. International Conference on Primary Health Care, Alma-Ata, USSR. USSR.
Hagen, Kirsten. 2009. “The ‘Livingstone Call for Action’: A Critical Analysis.” University of Utrecht. igitur-archive.library.uu.nl/student-theses/.
Kalibu Ministries. 2016. “Kalibu Elderly Clinic – Shekinah Ministries USA.” 2016. shekinahministryusa.org/outreaches/.
Kazeze, Zifa. 2008. “Social Protection and Ageing in Malawi.” Population Ageing in Malawi: Understanding Challenges, Responding to Opportunities, 41–56. www.fao.org/tempref/docrep/
Kendall, Jacob, and Philip Anglewicz. 2018. “Living Arrangements and Health at Older Ages in Rural Malawi.” Ageing and Society 38 (5): 1018–40. doi.org/10.1017/s0144686x16001422.
Makaula, Peter, Paul Bloch, Hastings T Banda, Grace Bongololo Mbera, Charles Mangani, Alexandra de Sousa, Edwin Nkhono, Samuel Jemu, and Adamson S Muula. 2012. “Primary Health Care in Rural Malawi - a Qualitative Assessment Exploring the Relevance of the Community-Directed Interventions Approach.” BMC Health Services Research 12 (1): 328. doi.org/10.1186/1472-6963-12-328.
Makwero, Martha T. 2018. “Delivery of Primary Health Care in Malawi.” African Journal of Primary Health Care & Family Medicine 10 (1). doi.org/10.4102/phcfm.v10i1.1799.
MoH. 2012. “Malawi Health Sector Strategic Plan 2011-2016.” https://doi.org/Malawi Health Sector Strategic Plan 2011 - 2016 - Country Planning ... www.nationalplanningcycles.org/
———. 2016. “Malawi Health Care System.” Government of the Republic of Malawi. 2016. www.health.gov.mw/index.php/.
———. 2017. “Health Sector Strategic Plan II (2017-2022).” Government of the Republic of Malawi. Malawi Health Sector Strategic Plan II 2017-2022 - Country Planning ... www.nationalplanningcycles.org/
Multani, Narinder Kaur, and Satish Kumar Verma. 2007. Principles of Geriatric Physiotherapy. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd. doi.org/10.5005/jp/books/10676.
National Center for Injury Prevention and Control. 2008. How to Develop Community-Based Fall Prevention Programs for Older Adults. Atlanta, GA: Centers for Disease Control and Prevention.
National Policy for Older Persons. 2016. Lilongwe, Malawi.
NSO. 2008. “2008 Population and Census Housing Results,” 1–23. www.nsomalawi.mw/images/stories/.
———. 2018. “2018 Malawi Population and Housing Census: Preliminary Report.”
Nyondo, Ephraim. 2014. “Does Malawi Care about Elderly.” National Publications Limited Online, February 7, 2014. mwnation.com/.
Twea, Brenda. 2016. “Health Woe for the Aged.” National Publications Limited Online, April 10, 2016. mwnation.com/health-woe-for-the-aged/.
United Nations. 2017. “UNdata Malawi Country Profile.” UNdata. 2017. http://data.un.org/CountryProfile.aspx?crName=malawi%0A
WHO. 2015. “World Report on Egeing and Health.” World Health Organization. Geneva. Switzerland.
———. 2018. “Comprehensive Analytical Profile: Malawi.” World Health Organization, African Health Observatory. 2018. www.aho.afro.who.int/profiles_information/
Author Bios

Charles Nyasa (BSc. PT, Hons) is a Malawian physiotherapist with experience in clinical elderly care. His research interests lie in the area of functional capacity testing and human anatomy. Currently, he is an assistant lecturer of human anatomy in the division of anatomy, department of biomedical sciences, University of Malawi, College of Medicine.
Email: This email address is being protected from spambots. You need JavaScript enabled to view it.

Anthony Mwakikunga (PhD, Anatomy) is a Senior Lecturer of human anatomy and Deputy Dean in the faculty of biomedical sciences and health professions, University of Malawi, College of Medicine. He is also a post-doctoral fellow at the school of anatomical sciences, University of Malawi, College of Medicine.

Enock Madalitso Chisati (MSc, Bed, DipEd) is a Senior Lecturer and head of the Department of Physiotherapy, University of Malawi, College of Medicine. His research interest is in the area of exercise physiology and sports sciences. Enock is a PhD fellow of the Consortium for Advanced Research Training in Africa (CARTA).