
Elderly care is no longer just a first world burden. The need for geriatric care excellence and services is growing every day. With the improvement and accessibility of medical services, and with the improvement of health states and increased life expectancy every day, this renders our elderly community a growing cohort in need of specialized care.
The era we are living in is becoming more and more dependent on accessibility and the value of time is increasing by the minute. Many pre-existing beliefs are being tested at the moment. It is hard to wrap your head around the development of television being the most popular distraction over the past 30 years and that now it is a dying luxury and totally replaced by on demand video streaming. The essence behind this is the developing human nature that has become all of a sudden "impatient" and needs instant gratification.
The value of time has also changed over the years. Long ago when man had to hunt for food, hunting came with its own recipe for patience. The more time moved on, the less patient we became. The expectations for achievement over one given unit of time has also grown consistently over time. Time to visit relatives was exchanged for long phone calls to pre-written texts. Time is becoming more and more valuable. The rising value of time had its impact on the general pace of life and on the approved sector of the day for organizational matters.
Although health is a priority and represents the biggest fear on the personal and population level, yet the amazing fact is that most health-related complications are caused by a delay in seeking help. This fact is strange in relation to the importance of the issue. In an attempt to justify this finding, I conducted a number of interviews with elderly people in the course of a study that was related to elderly suicide rates and underlying factors. The scope of the interview was to understand how much they value the determinants of the quality of their own lives. One of the rubrics used to measure the value of health was the delay time from the beginning of a symptom until professional help was sought. The mean time reported for this was 3.2 days which is a very high number when compared to critical times like the window between embolism and brain atrophy could be as short as 30 minutes.

Although determinants of health and a healthy life per the WHO are many and include overt factors like proper housing and prevalence of health-related habits, one of the important determinants is personal attitude towards symptoms. In Egypt we joke about being the country with 100 million physicians, not because this is an exaggeration of fact but because people take pride in "not needing" professional health advice. Everyone who has ever been prescribed an antibiotic once in their lives, has informally received a certification to consult and give "better than expert" advice. Although it is hard to assess the actual price of informal practices like these, it does not require a postgraduate degree to pick up on the threat of delays in seeking medical advice. The cost of care for complications in many health conditions has been studied and varies from condition to condition but the bottom line is that complications cost the health system a considerable amount of expenditure that can be saved and redirected to acute care or even to prevention.

In response to the general global culture of accessibility, health professionals and drivers of change in health care have to open their senses to new UBER reforms that change paradigms and the lens through which we define scopes of service. In one lifetime we moved from paper journals that we ordered and had to wait two weeks for, to the need for 5G speeds to download and upload effectively over the internet because dial in internet is no longer serving the need to be constantly connected. Reform in health care on the other hand is not moving at the same pace. Health care AI interventions have been designed around aid missions for the past 100 years with no real change in the structure other than the travel plans.
This has become rather strange and to be upfront about it reveals how deeply drowned we are as health professionals in our own "right answer" that we are not really open to innovation.
Let's be open
Reality is that we need to take care of people who cannot take care of themselves. We need to make sure people are safe and that they are receiving "approved" services. In an attempt to structure accessibility of health and find a seat for university-based vocational training in the informal community-based services that are already in play, came the idea of GranCare.

Prof. Hala Sweed Director ASU- Geriatric Hospital
GranCare is an application that allows caregivers to sign up and upload their training certificates onto a portal where the universities authorize them as licensed home care givers. Licensing is equivalent to a predefined number of training hours and face to face consultation that they have performed. When authorized, the caregivers become "licensed" to offer home care for elderly patients who are suffering from conditions that do not necessitate hospital transfer. Training includes the capacity to identify referable symptoms, offer primary non-invasive health services and offer nursing consultations and capacity to communicate effectively with the local hospital for better health advice. Prof. Hala Sweed, Chair of the Geriatric Department and the New Geriatric Hospital in Ain Shams University Faculty of Medicine, with her ongoing project for caregiver training and certification advocated for this initiative and adopted it as her upcoming community-oriented challenge. At the moment as a part of her FAIMER Regional Institute project, she is working on developing a certification program for caregivers and a whole system of licensing and re-licensing.
An additional component is that there will be an in-house regulating system for security related approvals and follow up. This will reduce the numbers of crimes committed against elderly from caregivers who have not had a security check and who feel they are not monitored.
Imagine an app on your phone where you "order" a caregiver to come check on your mother's urinary catheter and maybe empty it and change her intravenous line. Once you start ordering it locates you, identifies certified caregivers who are in your area and their time of availability. You can see their reviews and how many patients they attended to. You can see the last time they renewed their licensing and which university endorsed them. You can see their area of excellence. Now you can decide and book. Your community caregiver is now assigned to you through the service provider (GranCare) and in turn his/her services are liable to feedback, complaints, escalation, and praise on the other side of the spectrum. Eng. Ayman Farouk, IT expert, consultant, and Development Director at SEE, describes the innovative approach above and offers an in-depth vision regarding the utility of Blockchain in the initiative.

Eng. Ayman Farouk MSc. Cloud solutions
Director Technology and Development SE Egypt
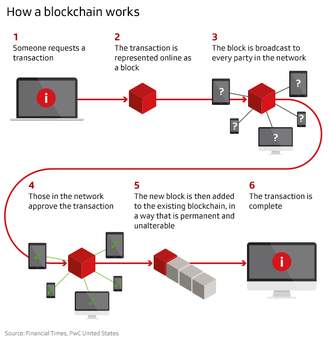
Blockchain as a technology can be used to ensure quality of product delivered through ensuring the quality of the chain of steps of manufacture, delivery, etc. When it used to build a secured automated market it provides services or products with a validated certificate of origin and quality of production through multilayer authorization.
The value of blockchain technology as a standardized authorization chain of process will lay the foundation of our solution. This is with reference to the similarity between production lines that produce an end product and the service that should be offered through our caregivers. In order to offer the best available service the following steps have to be ensured:
- Proper choice of candidate for service delivery (permission to join)
- Proper training
- Certification and authorization to provide the service
- Security check for candidates
- Records for time of availability and area of potential service
- Smart contracting for service delivery
- Follow up procedure for service
- Quality control procedures
- Improvement of service
This will limit third party beneficiaries in the middle of the two spectra of service. It will minimize unnecessary visits to the ER and outpatient clinics. It will limit the undesired effects of mobilizing elderly patients and faulty transfer. It will limit the need for existing on the streets during rush hours and office hours. This is in addition to the anticipated reduction in undesired health outcomes and complications and their attributed costs.
Now universities can finally find a community role that goes beyond the annual aid mission that is dispatched to the nearest rural area and is documented and shoved into a file for quality purposed and proof of adherence to our mission.
For funding purposes to implement this initiative we have enlisted the Gates Foundation through endorsement of the program The Middle East North Africa FAIMER Regional Institute. With expertise in KPI delivery and project advisors’ capacity in the area of ITC (Information Technology, and Communication), together with the appropriate funding we believe that GranCare can actually change the world of health care as we know it.
Learn more about ASUMENAFRI? here