
The authors state that there is no conflict of interest in this article.
This article is supported by the China Medical Board (CMB). Title of the project: “5+2+1 Joint Medical Education Model for General Practitioner. No.11-076.”
Abstract
Establishing a general practitioners’ system is a significant and difficult point of medical reform in China. The key problem of establishing a general practitioners’ system is that qualified general practitioners who have undergone the standardized training will be the gatekeepers of health. Presently, the general practitioners in China are short-handed and the training and employment of general practitioners is not keeping pace with need. This will cause an impasse in the establishment of a general practitioner system. There are many reasons for the impasse, but this paper argues that the core reason is the traditional pattern of interests is solidified and the new pattern of interests has not been established. The authors suggest that the government in the process of pushing grading diagnosis and treatment, could be refactoring the pattern of interests via fusion between Internet and medicine based on “Internet +” to reach a win-win situation in order to push the establishment of a general practitioner system.
Introduction
Primary healthcare systems mainly rely on general practitioners, health insurance, and health investment from government [1]. In order to improve China's primary health care system, in addition to reforming the government's health investment and medical insurance financing and paying mechanism, China has also continuously strengthened general medicine education and promoted the establishment of the general practitioner system, which has become one of the key issues of China's education and medical reform. The authors of this article attempt to analyze the predicament of the establishment of the general practitioner system in China and the practice of the Internet in the medical industry, combined with the characteristics of primary health care and "Internet +", to put forward the idea of promoting the establishment of a general practitioner system in China based on Internet technology.
Comparison of the General Practitioners in China and Beyond
The data from the website of Organization for Economic Co-operation and Development (OECD) and China Health and Family Planning Statistical Yearbook (2015) indicates the number of general practitioners per 1,000 in China is 0.14 which is lower than the United States (0.31), the United Kingdom (0.79), Israel (0.27), Turkey (0.57), and other countries. The proportion of general practitioners in China is 7.52 percent, which is also lower than the United States (11.89 percent), Canada (47.22 percent), Israel (8.67 percent), and other countries (Table 1) [2-3]. China still has a large gap in the number of general practitioners compared with other countries.
Table 1: Comparison on the General Practitioners between China and Others in 2015
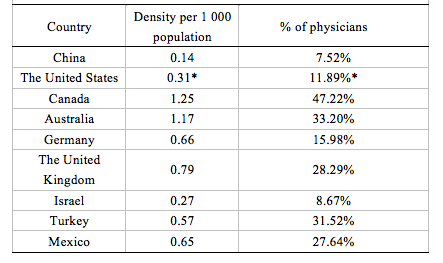
Note: Data from website of organization for Economic Co-operation and Development (OECD) and China Health and Family Planning Statistical Yearbook (2015)
*The data for The United States is for 2014
Comparison of Domestic General Practitioners
Comparing the number of general practitioners per 1,000 population in various provinces/municipalities/autonomous regions in China, the number of general practitioners per 1,000 in Beijing, Zhejiang, Shanghai, and Jiangsu was 0.38, 0.39, 0.30, and 0.26, respectively, which was significantly higher than the national average level (0.14). Guangdong Province, as a major economic province in China, has a total number of doctors per 1,000 population of only 0.14, which is equal to the national average level (Figure 1). Comparing the proportion of general practitioners who are qualified doctors, it is found that only Zhejiang, Jiangsu, Beijing, Guangdong, et al. are areas that have levels higher than the national average level (7.52 percent) (Figure2). Among the 31 provinces/municipalities/autonomous regions in China, only six provinces/municipalities/municipalities have a higher ratio of general practitioners per 1,000 population and 10 provinces/municipalities/practitioners higher than the national average level, which indicates that there are serious regional and structural imbalances in the distribution of GPs in China.
Figure 1: The number of general practitioners per 1,000 population in China, 2015
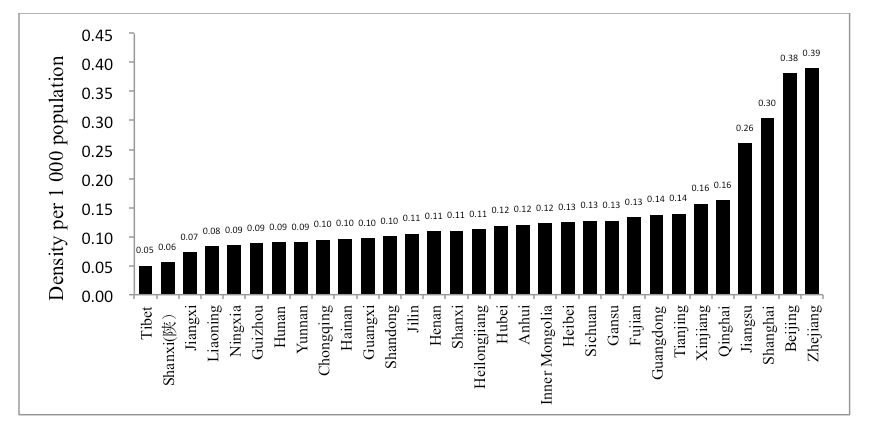
Note: Data from China Health and Family Planning Statistical Yearbook (2015)
Figure 2: The ratio between general practitioners and practicing physicians in China, 2013
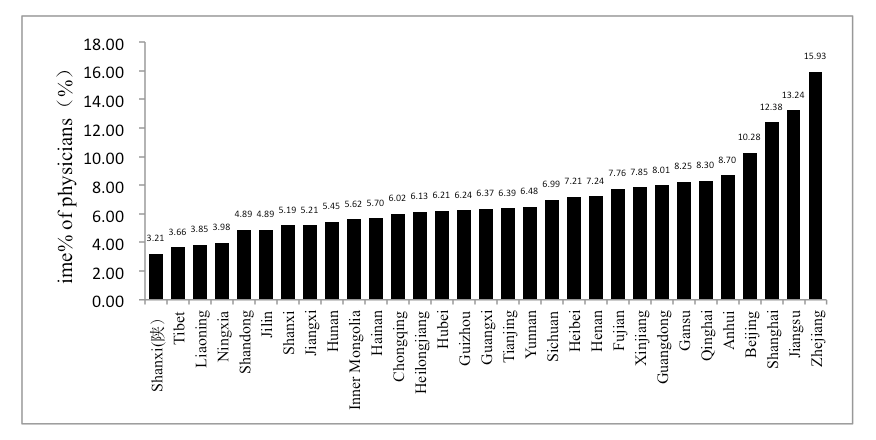
Note: Data from China Health and Family Planning Statistical Yearbook (2015)
In general, the number of general practitioners per 1,000 population and the proportion of general practitioners of qualified doctors in China are still far behind other countries. There is a serious shortage of general practitioner resources, imbalance in geographical distribution, and irrational proportion, which shows that the basic conditions for establishing a general practitioner system in China are poor.
Disconnect Between Training and Employment of General Practitioners
In recent years, in order to establish the general practitioner system, China has continuously improved the training system for general practitioners. In 2011, the “Guiding Opinions of the State Council on Establishing a General Practitioner System” pointed out that during the transitional period, the training mode of general practioners (GPs) in China is mainly the “3+2” training mode (i.e., after completing three years of medical education, continuing to participate in two years as an assistant general practitioner) and transfer training, and actively explore the standardized "5 + 3" training mode (i.e., after graduating from five years of medicine, participate in three years of standardized training for resident or postgraduate education for medicine).
According to statistics from the Guangdong General Hospital Education and Training Center, on January 11, 2016, the total number of postgraduates for general medicine in Guangdong Province was 22,766 of which 18,274 were certified, the number of transfer training for general practitioners was 2,783 of which 2,765 were certified, with 265 participating in standardized training for general practitioners in this center and 124 who actually obtained certificates, and the remaining 141 people who have not yet completed their studies. Currently the training model of general practitioners is mainly in-position and transfer training and the proportion of standardized training general practitioners is extremely low.
Guangzhou Medical University explores the “5+2+1” Master of Medicine joint training model under the state-designated “5+3” clinical medical personnel training model. The characteristics of this training model are as follows.
- Multinational: Teachers from home and abroad;
- Trans-sectoral: Cooperation between medical universities and Health and Family Planning Commission;
- Inter-disciplinary: Clinical medicine, preventive medicine, rehabilitation medicine, and other disciplines; and
- Emphasis on primary health center: focus on primary practice.
The first class enrolled in 2012 to the master’s in general medicine program and graduated successfully in June 2015 with only one student who chose to go to the primary healthcare institution for employment. Obviously, there is a serious disconnect between the training and employment of general practitioners.
Analysis
At present, China's general clinical medicine education has qualified training based on teachers’ resources. However, the greater challenge is that the training and employment of general practitioners continues to be out of line. General practitioners who undergo standardized training are reluctant to go into service for primary medical care, which also in turn hinders the development of general medical education, and eventually puts the establishment of the general practitioner system into a deadlock.
Reasons that result in training and employment of general practitioners are out of line including lack of professional honor, for example lower salary, poorer professional development prospects, and poor conditions in primary health service institutions. The main reason is the traditional pattern of interests that hinders the establishment of the general practitioner system.
Under the traditional pattern of medical interests, there are cross-cutting business relationships between different levels of health institutions. Hospitals and primary health care institutions have failed to form a collaboration relationship. With brand advantages, hospitals lack internal motivation to refer patients downwards; conversely, primary health care service providers are more willing to refer patients upwards due to insufficient service capacity and inadequate incentive mechanisms [4-5]. Moreover, design of the medical insurance system in China makes the difference in the cost of selecting service from hospitals and primary health care institutions not obvious and fails to exert effective and positive economic leverage in the establishment of a tiered health care delivery system [6-7]. At present, general practitioners have lower job satisfaction, weak will to service in primary health care institutions, and imperfections within their pension system, which results in a lack of enthusiasm for participating in establishment of the general practitioner system [8]. The establishment of the general practitioner system requires cooperation between hospitals and primary medical and health service institutions. Forming cooperating relationships needs government support, on the other hand, it requires hospitals and primary medical and health service institutions to actively participate [9]. Although the establishment of the general practitioner system was actively promoted, because of the uncoordinated interest mechanism under the traditional interest pattern, the hospital was in a position of interest monopoly, and the benefits of grassroots medical and health service institutions could not be guaranteed reasonably, resulting in hospitals and primary health care service institutions unwilling to establish the general practitioner system. General practitioners are reluctant to serve in the grassroots efforts, leading to the disconnect between training and employment of general practitioners, and hinderance of the establishment of the general practitioner system in China.
Establishment of General Practitioners’ System via Refactory of Interest Pattern Based on “Internet+”
On March 5, 2015, Li Keqiang, the prime minister of China proposed an "Internet Plus" action plan in the government work report in the third session of the Twelfth National People's Congress and raised it to the national strategic level. "Internet +" can break through the traditionally solidified interest pattern, refactor a new pattern of interests, achieve value-added benefits, and maintain multi-interest benefits, such as "Internet + traditional bazaar" derived Alibaba; "Internet + payment" derived Alipay; " and "Internet + private car" derived Uber.
The Internet has gradually been valued in the field of medical and health services
On March 30, 2015, the State Council issued the “Outline of the National Health Care Service System (2015-2020).” The document states that the healthy Chinese cloud service plan will be implemented and gradually change the mode of health services through the share of health information between all levels of health institutions. In the meantime, it makes full use of information communication technology to promote the vertical flow of medical resources and further promote the establishment and improvement of hierarchical medical treatment models. On July 1, 2015, the State Council "Guiding Opinions on Actively Promoting "Internet +" Action" put forward 11 action plans, of which the "Internet + Livelihood Service" action plan involves the health field and encourages the promotion of new online medical and health services through the development of Internet-based healthcare services. At present, the use of the Internet in the health field is gradually being considered, as most hospitals build the “WeChat” public platform to carry out information and expand function [10]. The hospital improved the patient consultation process through Internet technology, achieved zero queues for registered visits, improved patient experience, and improved hospital operating efficiency. The characteristics of “Internet+Health” can be summarized as follows: cross-border integration, interoperability, open-sharing, process transformation, and accuracy, all of which helps to break through the traditional pattern of interest by improving accessibility and fairness of medical services [11].
“Internet+ Health” Breaks Through the Traditional Pattern of Interest
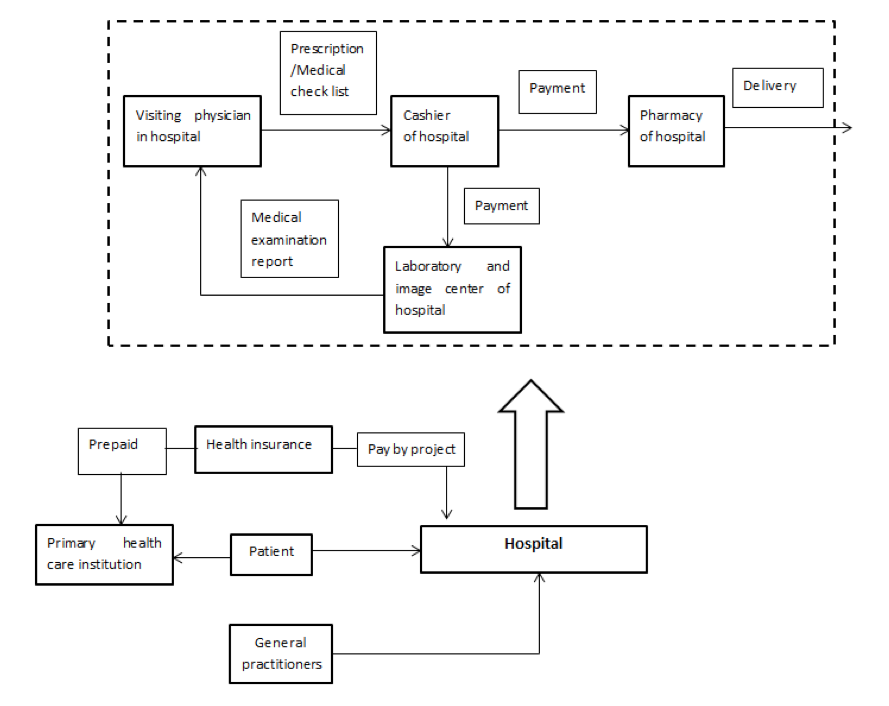
Under the traditional pattern of medical interests (Figure 3), government subsidies to hospitals are inadequate, and the hospital tends to be more profitable [12]. Hospitals and primary health care institutions form a competitive pattern. Hospitals collect health and high-quality hardware and software resources. That has prompted hospitals to be placed in interest monopolies under profit motives, which has ultimately led to the erosion of the interests of primary health care institutions so that general practitioners who have undergone standardized training have opted for employment in hospitals. However, further analysis found that the interests of hospitals, patients, and primary health care institutions under the traditional interest pattern were all damaged. First, hospital resources are too concentrated, which can easily lead to lower efficiency. Second, if all kinds of patients visit the hospital it would make the hospital overcrowded and increase operating costs. Third, patients have increased wait times for a visit and this would increase their time-cost. Fourth, the utilization rate of health resources in primary health care institutions is low, and it is difficult to exert its "six in one" function.
Figure 3: The traditional pattern of interests
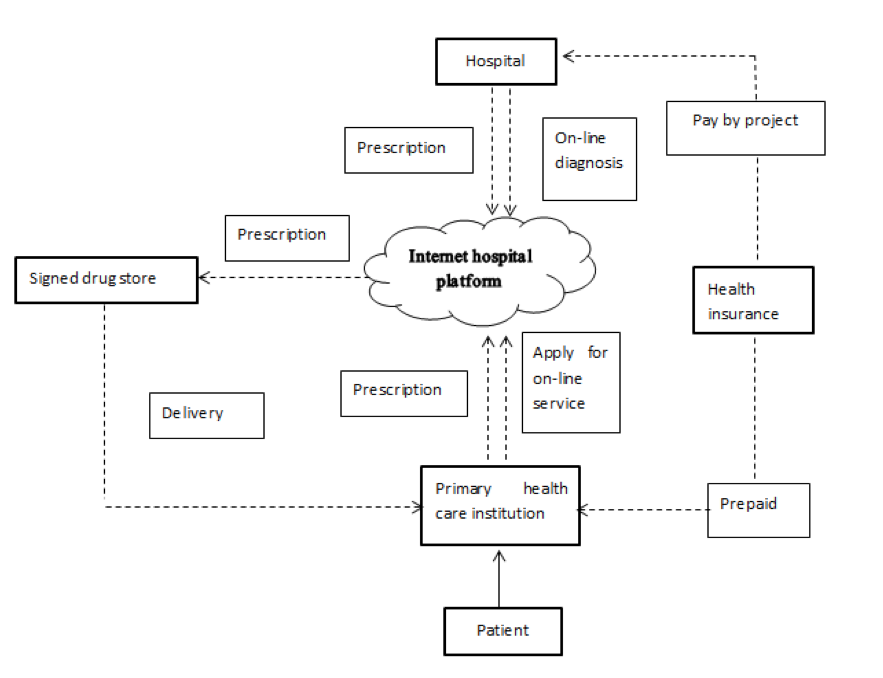
The first Internet hospital in Guangdong Province was officially opened on October 25, 2014. It mainly aims at diagnosis and treatment for common diseases and chronic diseases in remote areas by online health services. This new medical service model broke the old interest pattern and formed a new pattern of interests (Figure 4), achieving a win-win goal [13]. Residents signed contracts with village physicians, the number of people visiting the village clinics increased, additionally, salary, social recognition, and professional honor of the village physician increased. At the same time, medical technology training and guidance from large hospitals helped professional development of village physicians. Large hospitals extended outpatient clinics to the primary health care institution, stabilized patients that required hospitalization, reduced hospital operating costs, and increased hospital bed utilization rates; patients could receive medical services previously provided by large hospital experts in village clinics; pharmacies have a loyal customer base and were able to save in marketing costs.
Figure 4: The pattern of interests of the first internet hospital in Guangdong province
“Internet+ Health” Refactors a New Pattern of Interest
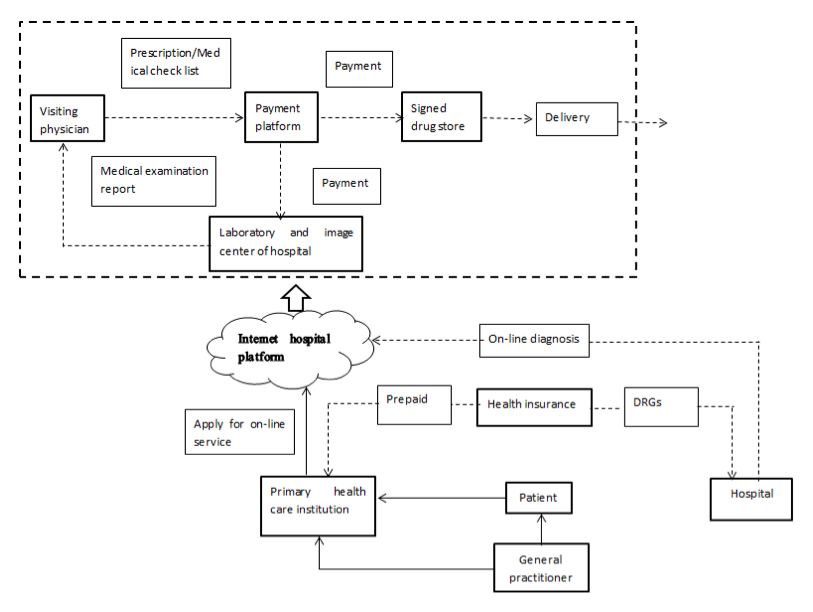
The following explores how to build a new Internet hospital platform based on "Internet +" and form a new interest pattern (see figure 5). First, general practitioners provide services to residents based on their contract. Medical insurance is prepaid according to the age, disease structure, and health status of residents signed with general practitioners. Secondly, the compensation mechanism of traditional medical insurance for hospitals is turned to DRGs. Third, under the promotion of the medical reform policy, the policy that eliminates the physicians profit from drugs will be carried out and the drugstore distribution mode implemented. Fourth, in order to share health information and reduce the operating costs of health institutions, medical imaging and other examinations are entrusted to third-party professional institutions. Under the new pattern of interest, interests for different interest subjects are as follows.
(1) Hospitals fix patient flow, improve hospital operating efficiency, and extend outpatient clinics to the community, hospitals and community general practitioners are responsible for the basic medical and health services of residents together;
(2) In the case of expanding outpatient care, the hospital stabilizes outpatient and inpatient flow, and can also conduct continuing education for general practitioners, as well as specialize in medical scientific research;
(3) Contracted pharmacies and third-party agencies have a fixed customer base to reduce the associated marketing costs;
(4) The service capabilities of primary health care institutions are improved. At the same time, patients can enjoy the medical services provided by experts from large hospitals at the primary health care institutions and reduce the opportunity cost for seeking medical attention.
Under the new medical service model, the function of a general practitioner as a health gatekeeper is reflected. First of all, the consultation is done by a general practitioner, if the disease diagnosis exceeds the competence of the general practitioner, online diagnosis can be conducted by connecting with the hospital through the internet hospital platform. Throughout the entire process of medical services, general practitioners and connecting hospitals receive performance awards based on the volume of contracts and the effectiveness of their services to share responsibility and benefit, thereby attracting general practitioners to take root in the primary health care institutions that will promote the establishment of the general practitioner system in China.
Figure 5: The new pattern of interests baded on "Internet+"
From the above, in the process of implementing a tiered health care delivery system, the government in China can build a new pattern of interests through a combination of the Internet and health care, connect all parties' interests with win-win results, boost the establishment of the general practitioner system, improve implementation of the tiered health care delivery model, and finally perfect the primary health care system.
Works Cited
[1] Huang MF, Wei DH, Rubino L, et al. " Three Pivots" of primary care system: a comparison between State of California in the United States and Guangdong Province in China [J]. Chinese General Practice, 2015, 18 (10) :1105-1108. (in Chinese)
[2] Organization for Economic Co-operation and Development. Health date [EB/OL]. [2016-1-5]. http://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_WFMI#.
[3] National Health and Family Planning Commission of the PRC. Chinese Health and Family Planning Yearbook [M]. Beijing: Peking Union Medical College Press, 2014. (in Chinese)
[4] Shen SG, Zhang B, Tiered health care delivery system, optional visiting and establishment primary health care institutions [J]. Academia Bimestrie, 2016, (02):48-57. (in Chinese)
[5] Xu D, Wang GB, Zhang M, et al. Present situation and strategies of collaboration-division between public hospitals and basic medical and health institutions [J]. Chinese Hospital Management, 2013,33(04):11-13. (in Chinese)
[6] Ma XJ, Dai T, Yang SX, et al. International experiences and implications of the practice and service mode of general practitioners [J]. Chinese Journal of Health Policy, 2015,8(02):13-18. (in Chinese)
[7] Yang XG, Ma XJ, Dai T. Influencing factors of the division and cooperation mechanism public hospitals and primary healthcare service institutions: A qualitative comparative analysis [J]. Chinese Journal of Health Policy, 2013, 6(08):14-19. (in Chinese)
[8] Chang X. Study on the relationship among job satisfaction, career burnout and intent to stay in general practitioners [D]. Shandong University, 2015. (in Chinese)
[9] Chen H, Wang XF. Conflict-cooperation relationship between hospitals and community health center based on F-H method [J]. System Engineering, 2015, 33(03):154-158. (in Chinese)
[10] Li DZ, Wei DH, Ding BF, et al. The discussion on the construction of hospital WeChat public platform under the Background of “Internet +” [J]. Chinese Hospitals, 2015, 19(8):60-63. (in Chinese)
[11] Li XH, Chen YB, Zhao X, et al. Internet + healthcare [M]. Beijing: People’s Medical Publishing House, 2015. (in Chinese)
[12] Li DZ, Wei DH, Wang LS, et al. Interests–oriented behavior of medical treatment and its restrictive mechanism from the perspective of economic man [J]. Medicine and Philosophy, 2015, 36(2a):68-70. (in Chinese)
[13] Tu J, Wang CX, Wu SL. The internet hospital: an emerging innovation in China [J]. The Lancet Global Health, 2015, 3(8): e445-e446.